Are you considering donating a kidney to a family member or friend?
If you are, This post is for you to help empower you to be a smart kidney donor.
Wanting to donate a kidney to improve or even save the life of another person suffering from kidney failure is a noble and honorable thing. The donation of a live kidney is the best option for the recipient compared to donation from a deceased person as it will last longer and work better if put in properly and taken good care of. It is also certainly offers the recipient of the kidney a better and longer life compared to continued dialysis.
However, the most important thing for you to know about kidney donation as a possible donor is that donation is not safe for everybody.
Your primary responsibility is to ensure that it is safe for you to donate a kidney.
The doctors primary responsibility to you as a potential donor is to help you determine if it is safe for you to donate and nothing else.
If you do not really want to be a donor for whatever reason, you should not be forced to do so. Talk to the doctor evaluating you as a donor in private and tell the doctor your concerns. Your doctor will be able to speak confidentially on your behalf and tell the person hoping to get the kidney from you that you are not medically fit to be a kidney donor. The doctor does not need to tell them of your fears or concerns unless you ask them to do so.
First things first – who can donate a kidney?
The person intending to donate a kidney generally should be healthy, be between the ages of 20 and 65, should have 2 kidneys, should not be obesse (defined as a body mass index of >30) and have none of the following.
1) kidney disease or kidney stones
2) high blood pressure or high blood sugar
3) Large amounts of protein or blood in the urine
4) Have normal liver, heart and blood vessel function.
5) Have no ongoing infections, cancers or bleeding issues
6) Be mentally stable
Many people assume that everybody has 2 kidneys. However, it is important to know that many people live normal healthy lives being born with one kidney as long as it doesn’t get diseased. It is estimated that as many as 1 in 1000 to 1 in 1500 (100,000 to 150,000 Nigerians) were born with one kidney so do not assume you have 2 kidneys and can donate.
Most kidney transplants in Nigeria are either from related or unrelated living persons that are ABO blood group compatible. This means that a person with blood group O can donate to a patient with any blood group. A person with blood group AB can only donate to persons with blood group AB, while people with blood group B can only donate to patients with blood group B. People with blood group A can donate only to patients with blood group A. In special circumstances of donor blood group type A2, donation to patients with blood group O, B and AB is possible but decisions for such need to be very carefully made. Transplant outside these assignments while possible is associated with a higher risk of rejection of the transplant by the recipient and requires more high risk treatments to the recipient such as removal of the spleen or treatment with strong medications. Rhesus blood group is not considered a barrier to kidney transplantation
Donor Testing
As a donor, you need testing done. This is to ensure the you are of the right blood group, you have 2 kidneys, you are healthy, can stand the stress of surgery and do not have silent kidney disease or conditions that can cause kidney disease as well. Testing is also necessary to ensure that you do not transmit infections or cancers to the recipient. A psychological evaluation may also be necessary to ensure you can withstand the emotional stresses that may come during and after kidney donation.
Special testing also needs to be done to ensure you and the recipient are compatible to avoid rejection and help the surgeons know which kidney to take out of the donor and how best to take it out. Some transplant centers require that a donor be related to the recipient while other transplant centers do not insist on such a relationship.
Donor Surgery
As a donor, you should also know who will be performing the surgery and what their track record is. Not all surgeons know how to take out a kidney for the purpose of kidney donation. Taking out the kidney for the purpose of kidney donation is very different from taking the kidney out because of kidney disease. The kidney for donation has to be very carefully handled and it needs to be done quickly with minimal injury to the patient. Therefore ensure your surgeon knows what he or she is doing. Kidney donation surgery can be done in two ways.
The more recent way of taking out the kidney is a more recent and less painful way and is called keyhole or laparoscopic surgery. With this approach, 3 small holes and a 2-3 inch incision are made in your abdomen to remove the kidney. The scars are small, after a while are difficult to see and the recovery time is short. The other way is by open surgery where a long incision 8 or more inches in length is made on your side to take out the kidney. More painful with a longer recovery. Whatever method is used, make sure that the surgeon knows what he is doing. Ask about their complication rates and how many of the procedures they have done to determine their level of experience. A confident doctor should be willing to tell you what you want to know.
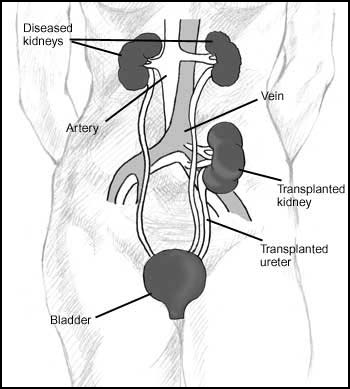
The decision to take out the right or the left kidney if prior testing is acceptable really depends on a number of factors that are best determined by the surgeon. However, in general, the right kidney is often selected for removal because it has a longer main artery and vein. Other considerations may make removal of the left kidney a better option.


Risks of kidney donation – short-term and long-term.
The whole point of testing to ensure that the donor is healthy and finding an experienced surgeon is to ensure that the risk of harm to the donor is as low as possible.
The first living donor kidney transplant was performed over 50 years ago and since then several thousand kidney donations from living persons have been performed. A vast majority of these donors have been doing well several years after donation so the consensus now is that in properly tested and selected donors, the long term outlook is very good. There is also experience from soldiers and other victims of war who were healthy but had to have one kidney removed because of war injuries. These otherwise healthy soldiers or victims of war have also been shown to live well without problems of kidney failure decades afterwards.
However, it is important to know that even if you have 2 kidneys, if you have risk factors for kidney disease or you are not selected properly for donation, you could have problems and possibly end up on dialysis or needing a transplant yourself.
If after you are evaluated and you are considered a good candidate and eventually donate , you need to follow a few simple rules to ensure all goes well in the long term
1) You must live a healthy life after kidney donation. This means you can not smoke, drink, add weight or engage in any other risky behaviours that could increase your risk for kidney disease.
2) You need to exercise and eat healthy continually.
3) You need to see a doctor at least once a year for the rest of your life. This is not because of a high concern for kidney disease. This is to help identify problems that might lead to kidney disease early so that progressive kidney disease can be treated and hopefully avoided.
Data from the United States shows that the risk of death within 90 days of living kidney donation is approximately 3 per 10,000 donor surgeries. This is better than the risk from laparoscopic gall bladder removal (18 per 10000 cases) or non donor nephrectomy (260 per 10,000). Other risks such as bleeding, infections, problems with wound healing etc occur at a rate of 2 to 5 per 100 cases. The incidence rates in Nigeria or other countries may be significantly different and data is not readily available on such.
The key long term concerns after donation are that of progressive and end stage kidney disease that might also require dialysis or transplant. Similarly, data from the United States and other developed countries show that the long term risk of developing kidney failure in properly selected donors who continue to maintain healthy lifestyle and habits is low.
General acceptability of kidney donation and kidney transplantation.
Some patients and their families may have concerns that it is religiously unacceptable to get a kidney transplant. The Catholic and Anglican Church, the major Islamic bodies and Jehovah’s Witness church have approved kidney transplantation from either cadaver or living donors. In the case of Jehovah witnesses, the organ is purged/flushed of all blood and transplantation without blood transfusion while risky is possible.
Disclaimer
This post is no substitute for an actual evaluation in a medical center by a qualified and experienced professional. This post is not a recommendation to come to KidneySolutions or any other specific medical center either.
This post is only meant to educate and empower potential donors so that the experience of kidney donation is not as frightening, evaluation is properly done and potential donors have an idea of what is going on.
Questions?
If you have any questions regarding kidney donation, feel free to fill the contact form below. We will endeavour to get back to you with answers as soon as possible.