
March 10th 2016 was world kidney day with a specific focus on childhood kidney disease.
Kidney disease affects millions of people worldwide, including many children who may be at risk at an early age. It is therefore crucial that we encourage and facilitate education, early detection and a healthy life style in children, to fight the increase of preventable kidney diseases and to treat children with inborn and acquired disorders of the kidneys worldwide.
Kidney disease can affect children in various ways, ranging from treatable disorders without long-term effects to life-threatening conditions. Acute kidney disease develops suddenly, lasts a short time, and can be serious with long-lasting effects or may go away completely once the underlying cause has been treated. Chronic kidney disease (CKD) does not go away with treatment and tends to get worse over time. CKD eventually leads to kidney failure, described as end-stage kidney disease or ESRD when treated with a kidney transplant or blood-filtering treatments called dialysis.
Children with CKD or kidney failure face many challenges, which can include
- a negative self-image
- relationship problems
- behavior problems
- learning problems
- trouble concentrating
- delayed language skills development
- delayed motor skills development
Children with CKD may grow at a slower rate than their mates, and urinary incontinence—the loss of bladder control, which results in the accidental loss of urine—is common.

Urinary tract inside the outline of the upper half of a human body. Every day, the two kidneys filter about 120 to 150 liters of blood to produce about 1 to 2 liters of urine, composed of wastes and extra fluid.
The kidneys are two bean-shaped organs, each about the size of a fist. They are located just below the rib cage, one on each side of the back. Every day, the two kidneys filter about 120 to 150 liters of blood to produce about 1 to 2liters of urine, composed of wastes and extra fluid. Children produce less urine than adults and the amount produced depends on their age. The kidneys work around the clock; a person does not control what the kidneys do. Ureters are the thin tubes of muscle—one on each side of the bladder—that carry urine from each of the kidneys to the bladder. The bladder stores urine until the person finds a time and place to urinate.
The kidney is not one large filter. Each kidney is made up of about a million filter units called nephrons. Each nephron filters a small amount of blood. The nephron includes a filter, called a glomerulus, and a tubule. The nephrons work through a two-step process. The glomerulus lets fluid and waste products pass through it; however, it prevents blood cells and large molecules, mostly proteins, from passing. The filtered fluid then passes through the tubule, which changes the fluid by sending needed minerals back to the blood and removing wastes. The final product becomes urine.
The kidneys also control the level of minerals such as sodium, phosphorus, and potassium in the body, and produce an important hormone to signal to the bone to create blood. A low level of red blood cells is called anemia and can be a result of kidney disease.

Picture above of a kidney with an inset of a nephron. Each kidney is made up of about a million filtering units called nephrons. Each nephron filters a small amount of blood. The nephron includes a filter, called a glomerulus, and a tubule.
What are the causes of kidney disease in children?
Kidney disease in children can be caused by
- birth defects
- hereditary diseases
- infection
- nephrotic syndrome
- systemic diseases
- trauma
- urine blockage or reflux
From birth to age 4, birth defects and hereditary diseases are the leading causes of kidney failure. Between ages 5 and 14, kidney failure is most commonly caused by hereditary diseases, nephrotic syndrome, and systemic diseases. Between ages 15 and 19, diseases that affect the glomeruli are the leading cause of kidney failure, and hereditary diseases become less common.
Birth Defects
A birth defect is a problem that happens while a baby is developing in the mother’s womb. Birth defects that affect the kidneys include renal agenesis, renal dysplasia, and ectopic kidney, to name a few. These defects are abnormalities of size, structure, or position of the kidneys:
- renal agenesis—children born with only one kidney
- renal dysplasia—children born with both kidneys, yet one does not function
- ectopic kidney—children born with a kidney that is located below, above, or on the opposite side of its usual position
- Some children are born without kidneys. They usually are born dead or die soon after birth
In general, children with these conditions except being born without kidneys lead full, healthy lives. However, some children with renal agenesis or renal dysplasia are at increased risk for developing kidney disease.
Hereditary Diseases: Hereditary kidney diseases are illnesses passed from parent to child through the genes. One example is polycystic kidney disease (PKD), characterized by many grapelike clusters of fluid-filled cysts—abnormal sacs—that make both kidneys larger over time. These cysts take over and destroy working kidney tissue.
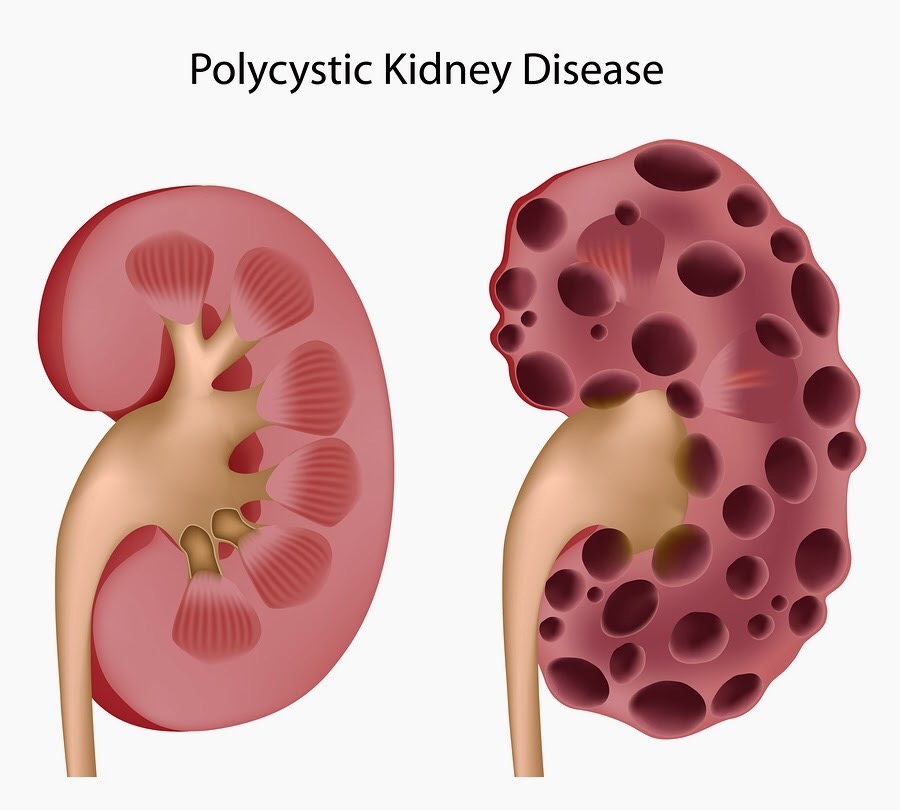
a picture of a normal kidney to the left and a diseased polycystic kidney on the right
Another hereditary disease is Alport syndrome, which is caused by a mutation in a gene for a type of protein called collagen that makes up the glomeruli. The condition leads to scarring of the kidneys. Alport syndrome generally develops in early childhood and is more serious in boys than in girls. The condition can lead to hearing and vision problems in addition to kidney disease.
Infection
Hemolytic uremic syndrome and acute post-streptococcal glomerulonephritis are kidney diseases that can develop in a child after an infection.
Hemolytic uremic syndrome is a rare disease that is often caused by the Escherichia coli (E. coli) bacterium found in contaminated foods, such as meat, milk products, and juice. Hemolytic uremic syndrome develops when E. coli bacteria lodged in the digestive tract make toxins that enter the bloodstream. The toxins start to destroy red blood cells and damage the lining of the blood vessels, including the glomeruli. Most children who get an E. coli infection have vomiting, stomach cramps, and bloody diarrhea for 2 to 3 days. Children who develop hemolytic uremic syndrome become pale, tired, and irritable. Hemolytic uremic syndrome can lead to kidney failure in some children.
Post-streptococcal glomerulonephritis can occur after an episode of strep throat or a skin infection. The Streptococcus bacterium does not attack the kidneys directly; instead, the infection may stimulate the immune system to overproduce antibodies. Antibodies are proteins made by the immune system. The immune system protects people from infection by identifying and destroying bacteria, viruses, and other potentially harmful foreign substances. When the extra antibodies circulate in the blood and finally deposit in the glomeruli, the kidneys can be damaged. Most cases of post-streptococcal glomerulonephritis develop 1 to 3 weeks after an untreated infection, though it may be as long as 6 weeks. Post-streptococcal glomerulonephritis lasts only a brief time and the kidneys usually recover. In a few cases, kidney damage may be permanent.
Nephrotic Syndrome
Nephrotic syndrome is a collection of symptoms that indicate kidney damage. Nephrotic syndrome includes all of the following conditions:
albuminuria—when a person’s urine contains an elevated level of albumin, a protein typically found in the blood
- hyperlipidemia—higher-than-normal fat and cholesterol levels in the blood
- edema—swelling, usually in the legs, feet, or ankles and less often in the hands or face
- hypoalbuminemia—low levels of albumin in the blood

child with swollen eyes and face from nephrotic syndrome affecting the kidneys
Nephrotic syndrome in children can be caused by the following conditions:
Minimal change disease is a condition characterized by damage to the glomeruli that can be seen only with an electron microscope, which shows tiny details better than any other type of microscope. The cause of minimal change disease is unknown; some health care providers think it may occur after allergic reactions, vaccinations, and viral infections.
Focal segmental glomerulosclerosis is scarring in scattered regions of the kidney, typically limited to a small number of glomeruli.
Membranoproliferative glomerulonephritis is a group of autoimmune diseases that cause antibodies to build up on a membrane in the kidney. Autoimmune diseases cause the body’s immune system to attack the body’s own cells and organs.
Systemic Diseases
Systemic diseases, such as systemic lupus erythematosus (SLE or lupus) and diabetes, involve many organs or the whole body, including the kidneys:
Lupus nephritis is kidney inflammation caused by SLE, which is an autoimmune disease.
Diabetes leads to elevated levels of blood glucose, also called blood sugar, which scar the kidneys and increase the speed at which blood flows into the kidneys. Faster blood flow strains the glomeruli, decreasing their ability to filter blood, and raises blood pressure. Kidney disease caused by diabetes is called diabetic kidney disease. While diabetes is the number one cause of kidney failure in adults, it is an uncommon cause during childhood.
Trauma: Traumas such as burns, dehydration, bleeding, injury, or surgery can cause very low blood pressure, which decreases blood flow to the kidneys. Low blood flow can result in acute kidney failure.
Urine Blockage or Reflux: When a blockage develops between the kidneys and the urethra, urine can back up into the kidneys and cause damage. Reflux—urine flowing from the bladder up to the kidney—happens when the valve between the bladder and the ureter does not close all the way.
How is kidney disease in children diagnosed?
A health care provider diagnoses kidney disease in children by completing a physical exam, asking for a medical history, and reviewing signs and symptoms. To confirm diagnosis, the health care provider may order one or more of the following tests:
Urine Tests
Dipstick test for albumin. The presence of albumin in urine is a sign that the kidneys may be damaged. Albumin in urine can be detected with a dipstick test performed on a urine sample. The urine sample is collected in a special container in a health care provider’s office or a commercial facility and can be tested in the same location or sent to a lab for analysis. With a dipstick test, a nurse or technician places a strip of chemically treated paper, called a dipstick, into the person’s urine sample. Patches on the dipstick change color when albumin is present in urine.
Urine albumin-to-creatinine ratio. A more precise measurement, such as a urine albumin-to-creatinine ratio, may be necessary to confirm kidney disease. Unlike a dipstick test for albumin, a urine albumin-to-creatinine ratio—the ratio between the amount of albumin and the amount of creatinine in urine—is not affected by variation in urine concentration.
Blood test: Blood drawn in a health care provider’s office and sent to a lab for analysis can be tested to estimate how much blood the kidneys filter each minute, called the estimated glomerular filtration rate or eGFR. This is a simple test not expensive and results can be available in a few hours
Imaging studies: Imaging studies provide pictures of the kidneys. The pictures help the health care provider see the size and shape of the kidneys and identify any abnormalities. This may be an ultrasound or CT scan or special type of x-ray
Kidney biopsy: Kidney biopsy is a procedure that involves taking a small piece of kidney tissue for examination with a microscope. Biopsy results show the cause of the kidney disease and extent of damage to the kidneys.
How is kidney disease in children treated?
Treatment for kidney disease in children depends on the cause of the illness. A child may be referred to a pediatric nephrologist—a doctor who specializes in treating kidney diseases and kidney failure in children—for treatment.
Children with a kidney disease that is causing high blood pressure may need to take medications to lower their blood pressure. Improving blood pressure can significantly slow the progression of kidney disease. The health care provider may prescribe
angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) which help relax blood vessels, reduce blood pressure and make it easier for the heart to pump blood
diuretics, medications that increase urine output and reduce body swelling
Many children require two or more medications to control their blood pressure; other types of blood pressure medications may also be needed.
As kidney function declines, children may need treatment for anemia and growth failure. Anemia is treated with a hormone called erythropoietin, which stimulates the bone marrow to produce red blood cells. Children with growth failure may need to make dietary changes and take food supplements or growth hormone injections.
Children with kidney disease that leads to kidney failure must receive treatment to replace the work the kidneys do. The two types of treatment are dialysis and transplantation.
Birth Defects: Children with renal agenesis or renal dysplasia should be monitored for signs of kidney damage. Treatment is not needed unless damage to the kidney occurs.
Ectopic kidney does not need to be treated unless it causes a blockage in the urinary tract or damage to the kidney. When a blockage is present, surgery may be needed to correct the position of the kidney for better drainage of urine. If extensive kidney damage has occurred, surgery may be needed to remove the kidney.
Hereditary Diseases: Children with PKD tend to have frequent urinary tract infections, which are treated with bacteria-fighting medications called antibiotics. PKD cannot be cured, so children with the condition receive treatment to slow the progression of kidney disease and treat the complications of PKD.
Alport syndrome also has no cure. Children with the condition receive treatment to slow disease progression and treat complications until the kidneys fail.
Infection: Treatment for hemolytic uremic syndrome includes maintaining normal salt and fluid levels in the body to ease symptoms and prevent further problems. A child may need a transfusion of red blood cells delivered through an intravenous (IV) tube. Some children may need dialysis for a short time to take over the work the kidneys usually do. Most children recover completely with no long-term consequences.
Children with post-streptococcal glomerulonephritis may be treated with antibiotics to destroy any bacteria that remain in the body and with medications to control swelling and high blood pressure. They may also need dialysis for a short period of time.
Nephrotic Syndrome: Nephrotic syndrome due to minimal change disease can often be successfully treated with corticosteroids. Corticosteroids decrease swelling and reduce the activity of the immune system. The dosage of the medication is decreased over time. Relapses are common; however, they usually respond to treatment. Corticosteroids are less effective in treating nephrotic syndrome due to focal segmental glomerulosclerosis or membranoproliferative glomerulonephritis. Children with these conditions may be given other immunosuppressive medications in addition to corticosteroids. Immunosuppressive medications prevent the body from making antibodies.
Systemic Diseases.
Lupus nephritis is treated with corticosteroids and other immunosuppressive medications. A child with lupus nephritis may also be treated with blood pressure-lowering medications. In many cases, treatment is effective in completely or partially controlling lupus nephritis.
Diabetic kidney disease usually takes many years to develop. Children with diabetes can prevent or slow the progression of diabetic kidney disease by taking medications to control high blood pressure and maintaining normal blood glucose levels.
Trauma: The types of trauma described above can be medically treated, though dialysis may be needed for a short time until blood flow and blood pressure return to normal.
Urine Blockage and Reflux: Treatment for urine blockage depends on the cause and severity of the blockage. In some cases, the blockage goes away without treatment. For children who continue to have urine blockage, surgery may be needed to remove the obstruction and restore urine flow. After surgery, a small tube, called a stent, may be placed in the ureter or urethra to keep it open temporarily while healing occurs.
Treatment for reflux may include prompt treatment of urinary tract infections and long-term use of antibiotics to prevent infections until reflux goes away on its own. Surgery has also been used in certain cases.

Eating, Diet, and Nutrition
For children with CKD, learning about nutrition is vital because their diet can affect how well their kidneys work. Parents or guardians should always consult with their child’s health care team before making any dietary changes. Staying healthy with CKD requires paying close attention to the following elements of a diet:
Protein. Children with CKD should eat enough protein for growth while limiting high protein intake. Too much protein can put an extra burden on the kidneys and cause kidney function to decline faster. Protein needs increase when a child is on dialysis because the dialysis process removes protein from the child’s blood. The health care team recommends the amount of protein needed for the child. Foods with protein include
- eggs
- milk
- cheese
- chicken
- fish
- red meats
- beans
- yogurt
- cottage cheese
Sodium. The amount of sodium children need depends on the stage of their kidney disease, their age, and sometimes other factors. The health care team may recommend limiting or adding sodium and salt to the diet. Foods high in sodium include
- canned foods
- some frozen foods
- most processed foods
- some snack foods, such as chips and crackers
Potassium. Potassium levels need to stay in the normal range for children with CKD, because too little or too much potassium can cause heart and muscle problems. Children may need to stay away from some fruits and vegetables or reduce the number of servings and portion sizes to make sure they do not take in too much potassium. The health care team recommends the amount of potassium a child needs. Low-potassium fruits and vegetables include
- apples
- cranberries
- strawberries
- blueberries
- raspberries
- pineapple
- cabbage
- boiled cauliflower
- mustard greens
- uncooked broccoli
High-potassium fruits and vegetables include
- oranges
- melons
- apricots
- bananas
- potatoes
- tomatoes
- sweet potatoes
- cooked spinach
- cooked broccoli
Phosphorus. Children with CKD need to control the level of phosphorus in their blood because too much phosphorus pulls calcium from the bones, making them weaker and more likely to break. Too much phosphorus also can cause itchy skin and red eyes. As CKD progresses, a child may need to take a phosphate binder with meals to lower the concentration of phosphorus in the blood. Phosphorus is found in high-protein foods. Foods with low levels of phosphorus include
- liquid non milk creamer
- green beans
- popcorn
- unprocessed meats from a butcher
- lemon-lime soda
- root beer
- powdered iced tea and lemonade mixes
- rice and corn cereals
- egg white
- sorbet
Fluids. Early in CKD, a child’s damaged kidneys may produce either too much or too little urine, which can lead to swelling or dehydration. As CKD progresses, children may need to limit fluid intake. The health care provider will tell the child and parents or guardians the goal for fluid intake.

Kidney disease, children and the responsibility we have to protect them. The two purple colored images on the back of the little baby boy below with yellow lines represent the kidneys. To learn more about kidney disease, visit us at www.kidney-solutions.com/faq
#kidney #kidneydisease #kidneyfailure #hemodialysis #kids #children #childhoodkidneydisease #transplant #peritonealdialysis


Thank you for informing about childhood kidney disease. I was incorrectly diagnosed with Polycystic Kidney Disease at age 16. At age 19, I was finally diagnosed with Medullary Cystic Kidney Disease. Going through high school with the complications of Chronic Kidney Disease was particularly challenging.
Best wishes,
Lauren
diphthongdays.wordpress.com
LikeLike